HomeReferrersRole of hybrid FDG PET/contrast CT parameters at early restaging for subsequent response to immunotherapy in advanced NSCLC
Role of hybrid FDG PET/contrast CT parameters at early restaging for subsequent response to immunotherapy in advanced NSCLC
26/10/2022
Dr Dalveer Singh MBBS (Hons), FRANZCR, FAANMS Qscan Radiology Clinics, UQ School of Medicine
Aim
We investigate whether clinically applicable semi-quantitative parameters derived from hybrid FDG PET diagnostic contrast enhanced CT (FDG PET/CECT) can predict immunotherapy treatment response in non-small cell lung cancer (NSCLC) patients.
The secondary aim was to assess the relationship of immune-related adverse events (irAEs) and metabolic activation of lymphoid cell-rich organs activation to response in patients continuing immunotherapy.
Method
Thirty-two patients who underwent hybrid FDG PET/CECT before and at first restaging after starting immunotherapy, with a minimum 12 months of 3-monthly FDG PET/CECT, were retrospectively analysed.
These PET-derived parameters were correlated to responding or stable disease as assessed by both RECIST 1.1 and iRECIST 1.1. IrAEs, if present, were also described and correlated with clinical benefit as determined by continuation of therapy by the oncologist. SUVmax of the spleen and bone marrow (as indicators of activation of lymphoid cell-rich organs) at restaging scans were also correlated to clinical benefit.
Results
Of 32 eligible patients, 10 (31%) experienced iCPD, 8 (25%) showed iSD, 9 (28%) had iPR and 5 (16%) had iCR. ΔSUVmaxTL (p = 0.008) and ΔSUVmaxnode (p < 0.001) were significantly associated with iPD vs. non-iPD. The presence of irAEs or spleen/marrow activation were not correlated to response rates.
Discussion
We describe semi-quantitative parameters on FDG PET/CECT by using the early interval metabolic delta and baseline necrosis as potential clinically useful and practical tools for immunotherapy treatment response evaluation in NSCLC.
The magnitude of change in SUVmax in the target tumour lesion (primary tumour) and the most intensely FDG avid nodal metastasis is significantly predictive of response to immunotherapy at 12 months of follow-up in lung cancer.
Whilst tumour necrosis was positively associated as a trend, we did not find this statistically significant in this cohort.
However, further larger volume studies may prove interesting as tumour necrosis can indicate a possibly responsive tumour microenvironment.
Hybrid contrast enhanced CT with PET imaging in lung cancer allows for extraction of clinically useful semi-quantitative parameters to aid clinical decision making in patients treated with immunotherapy.
Conclusion
Metabolic activation of spleen/marrow from immunotherapy and irAEs in patients deriving continued clinical benefit were not significant factors influencing response.
Figures
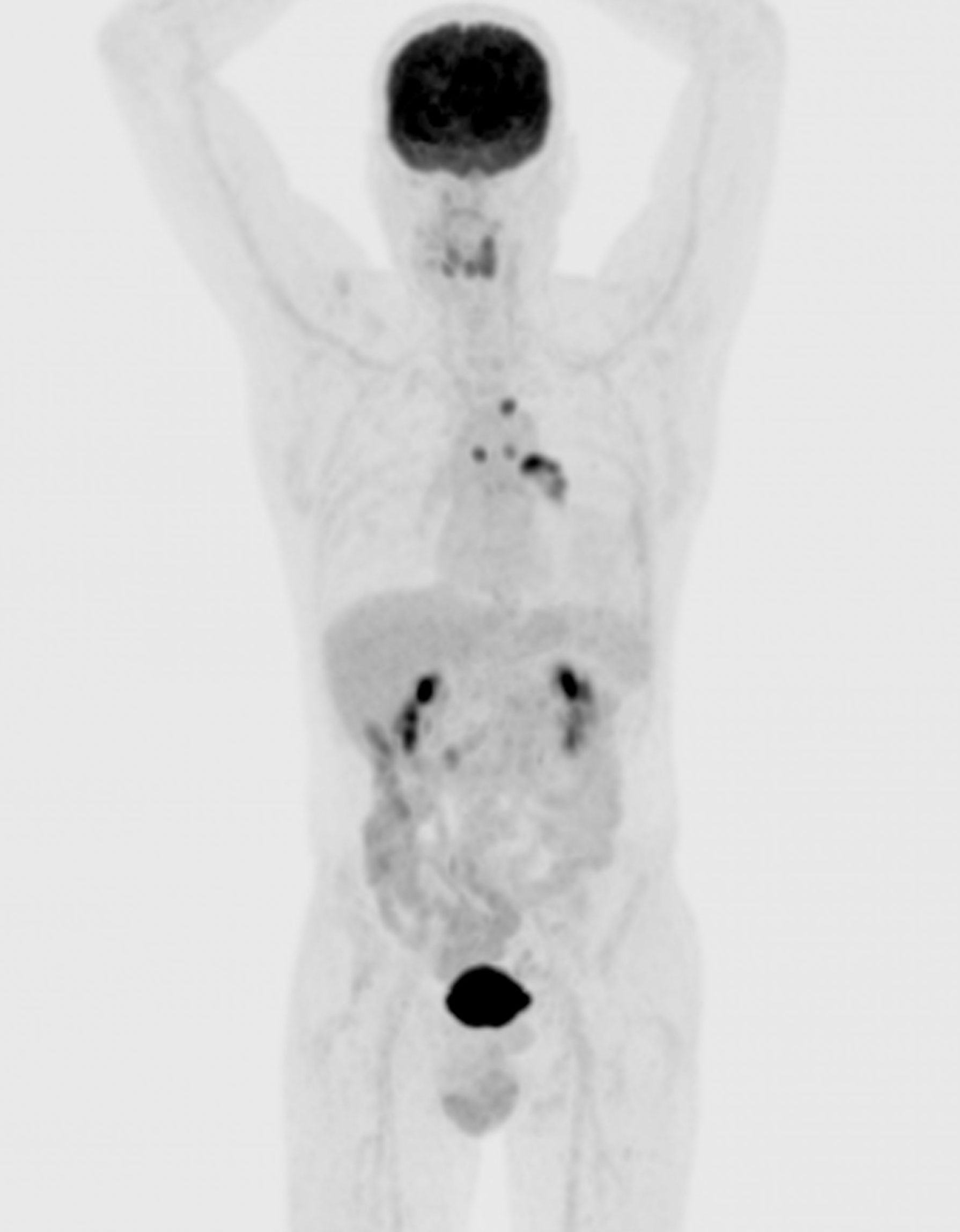
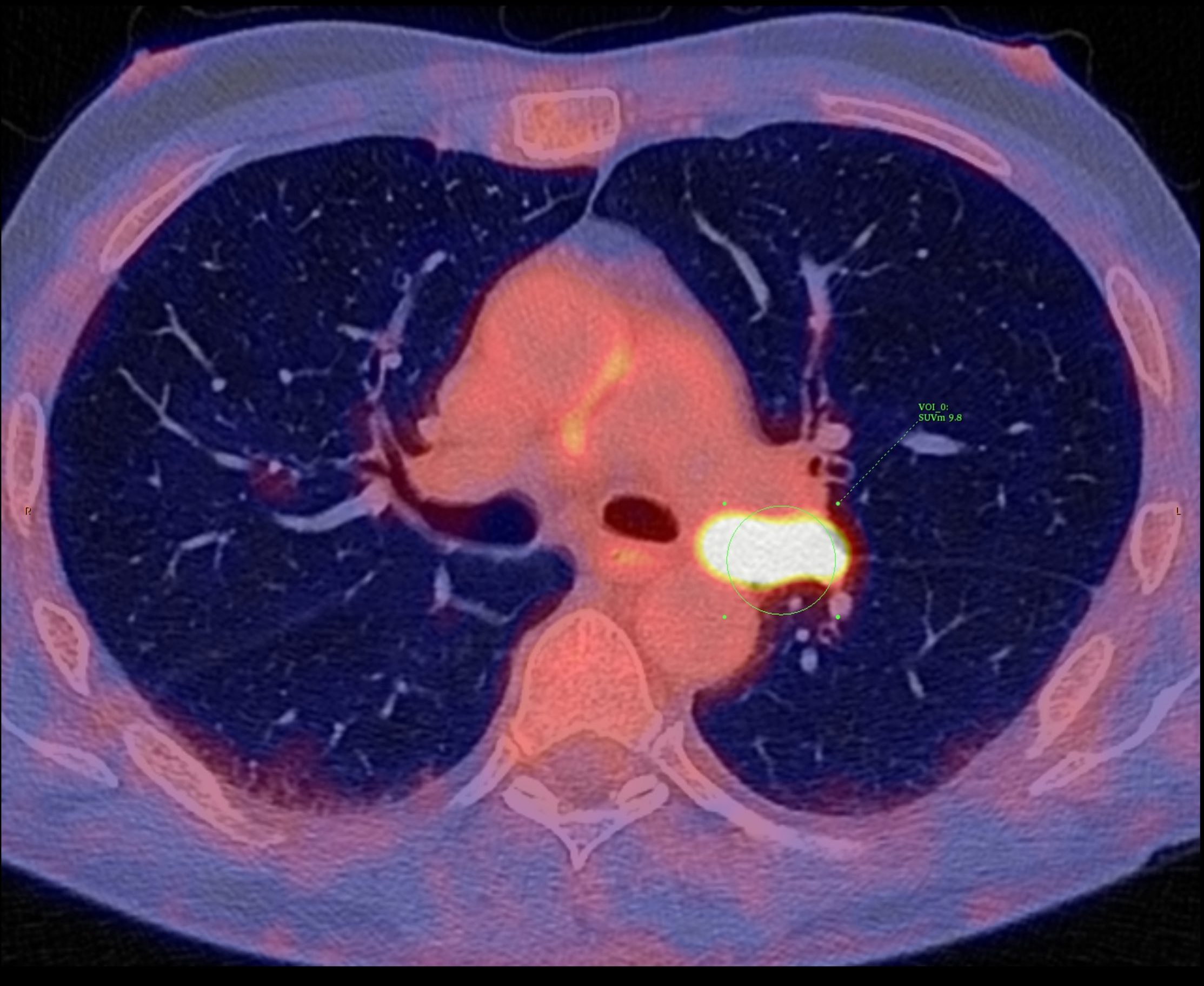
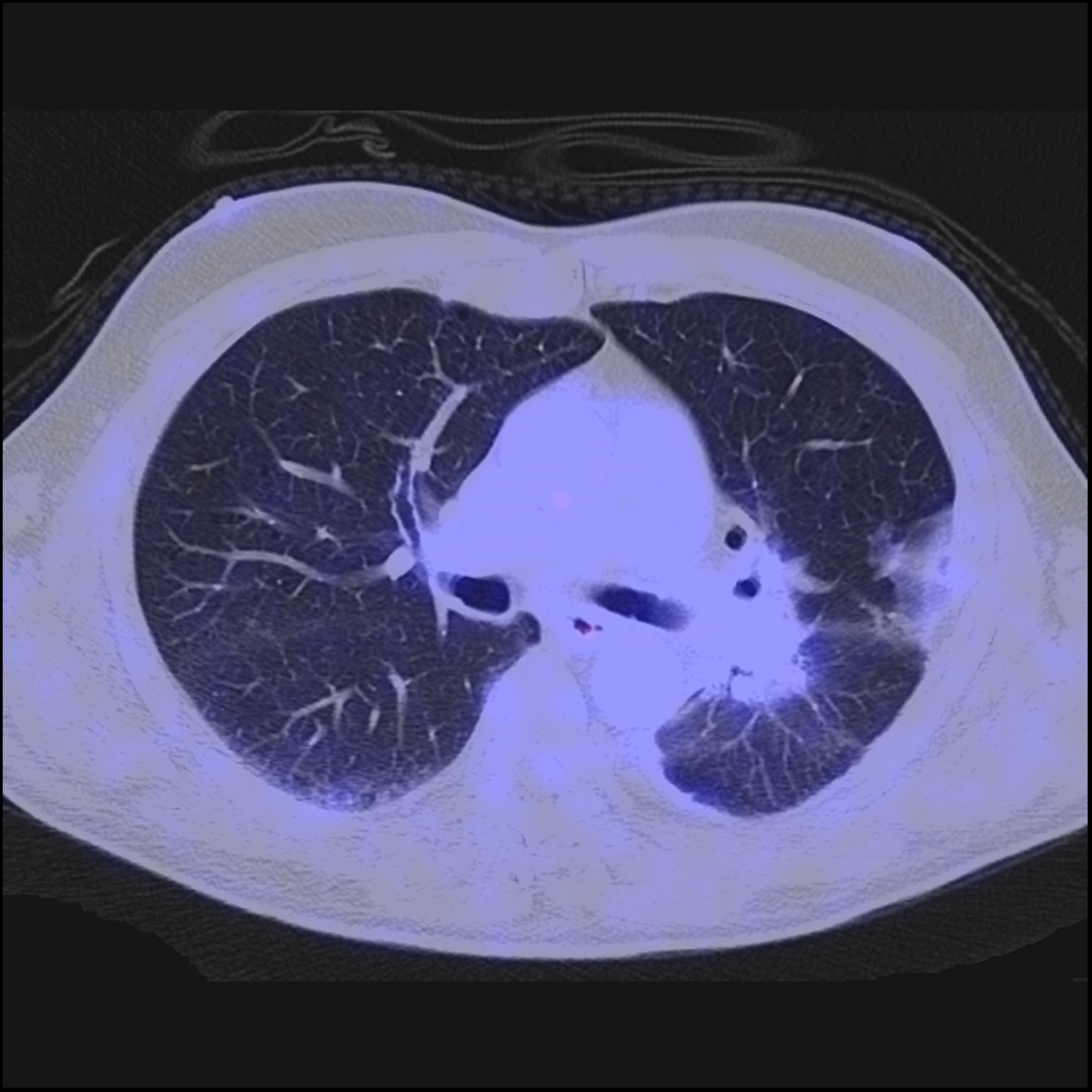
Figure 1A: 70M with NSCLC adenocarcinoma, left hilar primary tumour. Pre-treatment FDG PET/CECT shows intensely avid tumour, nodal and contralateral lung metastases. Tumour necrosis not a significant component in this case. Initial 3-month initial restaging PET/ CECT showed SUVmax reduction from 9.8 to 4.4 (>50%).
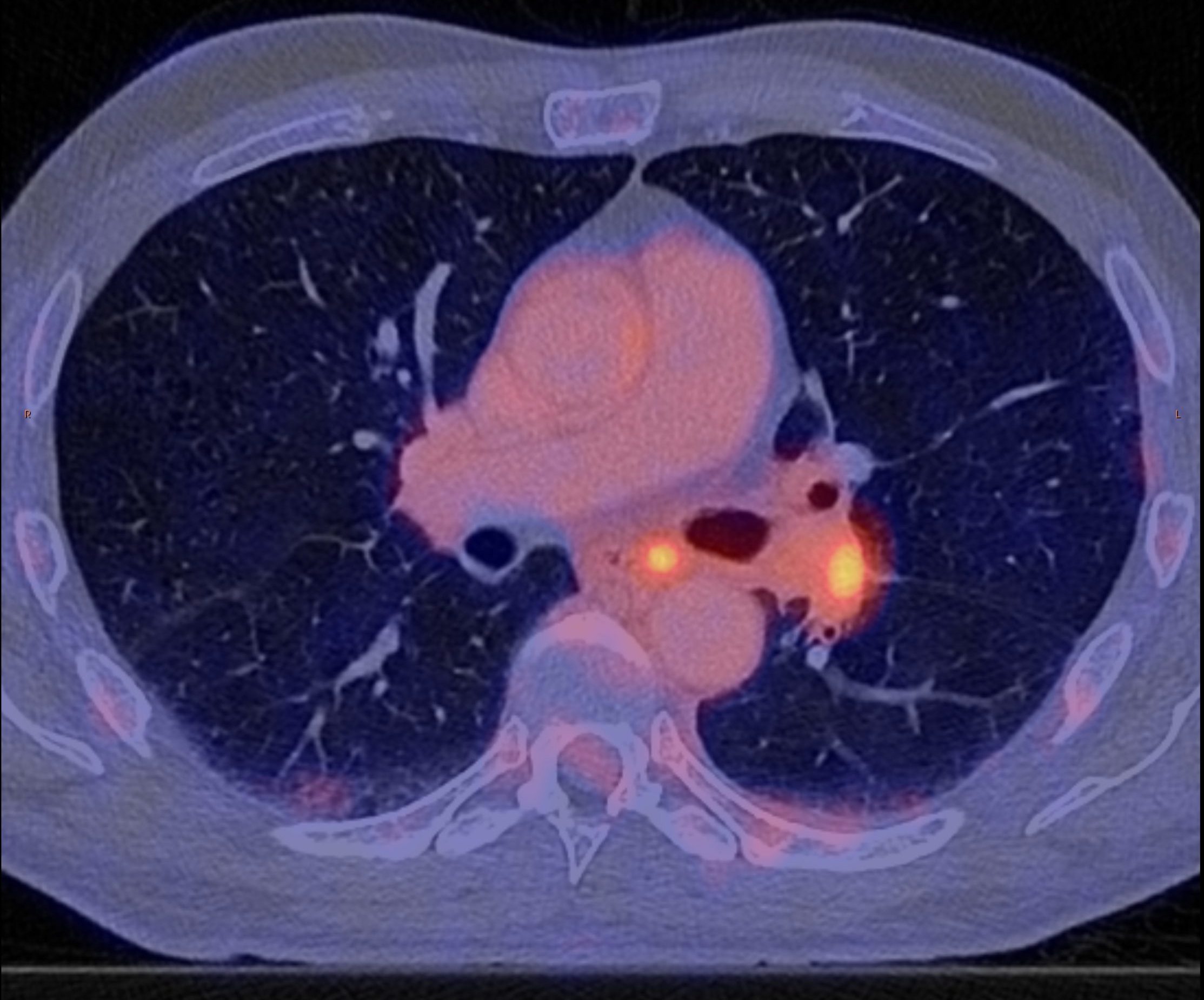
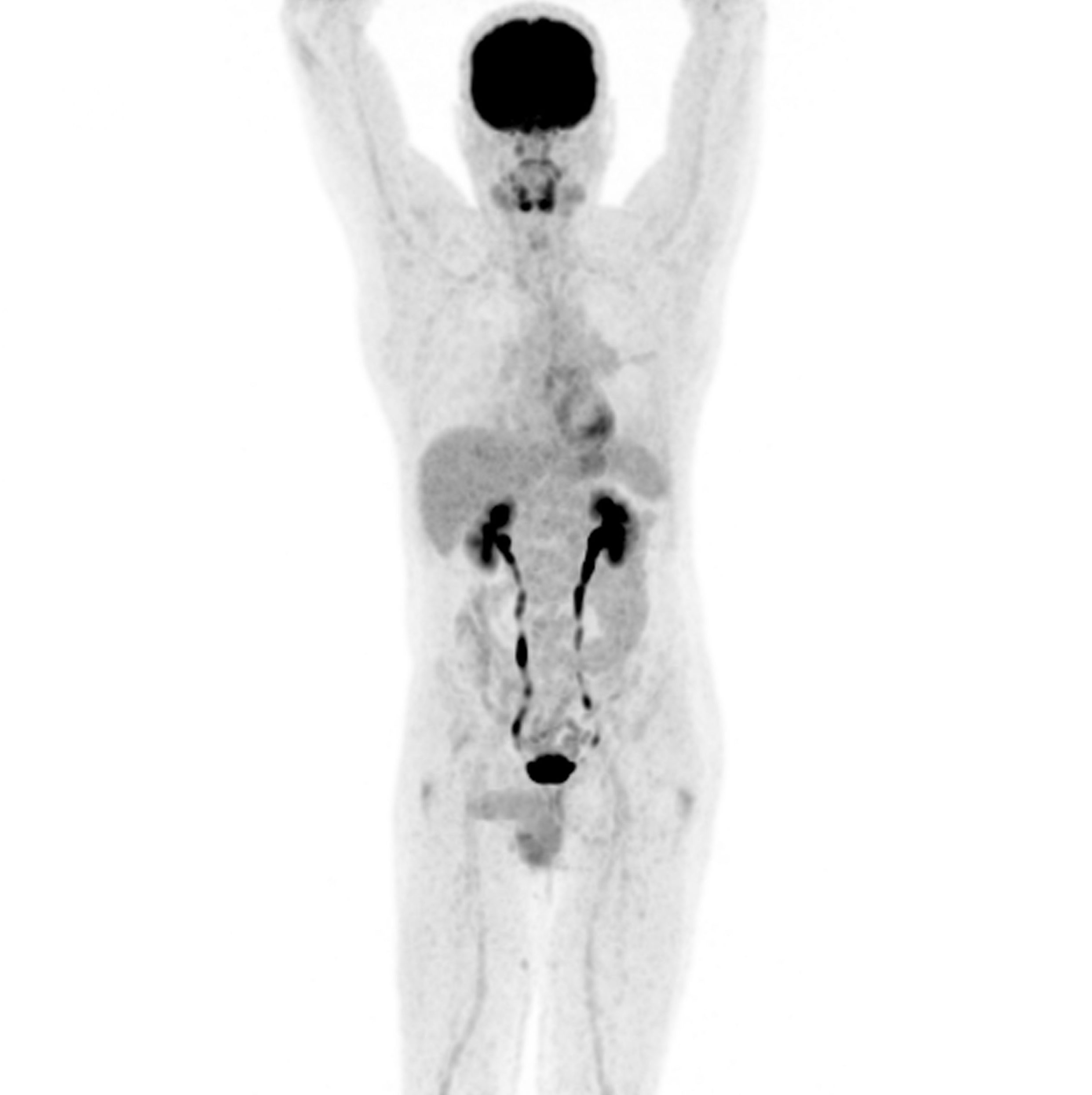
Figure 1B: At 12 months of follow-up, this patient shows complete sustained metabolic response to therapy. The magnitude of SUVmax response for the primary tumour and dominant node at the initial 3-month initial restaging PET/CECT study correlated to longterm immunotherapy response in this cohort.
References
Ferrari, C. et al. Immune Checkpoint Inhibitors in Advanced NSCLC: FDG PET/CT as a Troubleshooter in Treatment Response. Diagnostics 2021, 11, 1681. Curabitur ullamcorper ultricies nisi. Nam eget dui.
Lopci, E. et al. PET/CT Variants and Pitfalls in Lung Cancer & Mesothelioma. Sem Nuc Med 2021 51: 458-473.