Qscan Windsor will soon be home to the Philips MR7700 3T with Ambient Experience, the most advanced clinical MRI in the Southern Hemisphere.
This MRI’s features include:
Highest quality diffusion MRI imaging for all anatomies
Unmatched performance and precision, allowing for confident diagnoses
Patient-centred productivity, including freedom in patient positioning
A 70cm wide bore – the widest bore available
An in-bore solution, which leads to a decrease in levels of anxiety
Benefits of the Ambient Experience
The Ambient Experience integrates architecture, design, and enabling technologies to maximise patient comfort. In-bore video, dynamic lighting, side wall projection, and sound provide positive distractions for patients, who are also able to personalise their environment by selecting their own room themes and audio.
The Ambient Experience in-bore Connect provides the patient with information and guidance during the scan. It is an immersive video experience, with cues for breath holds and a personalised progress bar.
A study at the Herlev Gentofte University Hospital in Denmark found the in-bore experience led to a 70% reduction in interrupted exams. Patients felt more comfortable during and were more satisfied with their exams, and 84% reported that the progress bar helped them feel calmer during the scan.
The Philips MR7700 3T with Ambient Experience is now available at Qscan Windsor, with extended opening hours for MRI scans. Click here for more information about Qscan Windsor.
References
de Ruyter, B., & Timmers, I. (2020). The cost of fear and anxiety in radiology: What you can do to reduce it [White paper]. Koninklijke Philips N.V. https://www.usa.philips.com/healthcare/ consulting/articles/white-paper/ cost-of-fear-and-anxiety-inradiology
Women’s imaging encompasses a range of modalities, including
mammogram, breast ultrasound, breast MRIs, obstetric and gynaecologic MRIs.
Mammography is dedicated x-ray of the breasts, and can be
performed in asymptomatic women (screening mammogram) or those with symptoms
(diagnostic mammogram). Ultrasound is generally considered complementary to
mammography, and may be performed for assessment of an area of potential
abnormality seen on mammogram, or to ensure the breast tissue is normal.
In some women (such as those under the age of 35, or when pregnant/lactating),
ultrasound is recommended as a first line investigation. An ultrasound-
or mammographic-guided biopsy may be conducted if a radiologist requires a
sample of breast tissue for pathologic examination.
While mammograms and breast ultrasounds are primarily
concerned with the structure of breast tissue, MRI permits radiologists to
assess the function of the tissue (i.e. the physiology). Breast MRI is performed
for specific indications, such as for surgical planning, and for screening in
high risk populations (i.e. inherited genetic mutations).
Obstetric ultrasounds are performed as routine checkups for mother and baby. These may include early dating, nuchal translucency, morphology, and third trimester ultrasounds. Nuchal translucency ultrasounds are particularly important, as they can identify a pregnancy with an increased chance of chromosomal abnormalities – this includes Down syndrome, Patau syndrome, and Edwards’ syndrome.
Pelvic MRIs may be useful in the diagnosis of endometriosis or other fertility-related issues. It provides an image of the organs inside the pelvis, and is able to provide additional information regarding possible endometrial growths. They are also conducted if there is unexplained infertility or pelvic pain, can detect fibroids, and are useful for further investigation of pelvic masses and abnormal vaginal bleeding.
The newly re-opened Qscan Windsor clinic offers comprehensive women’s imaging services, including mammograms and mammogram-guided biopsies.
To book an appointment at Qscan Windsor, click here.
Dr Dalveer Singh MBBS (Hons), FRANZCR, FAANMS Qscan Radiology Clinics, UQ School of Medicine
Aim
We investigate whether clinically applicable semi-quantitative parameters derived from hybrid FDG PET diagnostic contrast enhanced CT (FDG PET/CECT) can predict immunotherapy treatment response in non-small cell lung cancer (NSCLC) patients.
The secondary aim was to assess the relationship of immune-related adverse events (irAEs) and metabolic activation of lymphoid cell-rich organs activation to response in patients continuing immunotherapy.
Method
Thirty-two patients who underwent hybrid FDG PET/CECT before and at first restaging after starting immunotherapy, with a minimum 12 months of 3-monthly FDG PET/CECT, were retrospectively analysed.
These PET-derived parameters were correlated to responding or stable disease as assessed by both RECIST 1.1 and iRECIST 1.1. IrAEs, if present, were also described and correlated with clinical benefit as determined by continuation of therapy by the oncologist. SUVmax of the spleen and bone marrow (as indicators of activation of lymphoid cell-rich organs) at restaging scans were also correlated to clinical benefit.
Results
Of 32 eligible patients, 10 (31%) experienced iCPD, 8 (25%) showed iSD, 9 (28%) had iPR and 5 (16%) had iCR. ΔSUVmaxTL (p = 0.008) and ΔSUVmaxnode (p < 0.001) were significantly associated with iPD vs. non-iPD. The presence of irAEs or spleen/marrow activation were not correlated to response rates.
Discussion
We describe semi-quantitative parameters on FDG PET/CECT by using the early interval metabolic delta and baseline necrosis as potential clinically useful and practical tools for immunotherapy treatment response evaluation in NSCLC.
The magnitude of change in SUVmax in the target tumour lesion (primary tumour) and the most intensely FDG avid nodal metastasis is significantly predictive of response to immunotherapy at 12 months of follow-up in lung cancer.
Whilst tumour necrosis was positively associated as a trend, we did not find this statistically significant in this cohort.
However, further larger volume studies may prove interesting as tumour necrosis can indicate a possibly responsive tumour microenvironment.
Hybrid contrast enhanced CT with PET imaging in lung cancer allows for extraction of clinically useful semi-quantitative parameters to aid clinical decision making in patients treated with immunotherapy.
Conclusion
Metabolic activation of spleen/marrow from immunotherapy and irAEs in patients deriving continued clinical benefit were not significant factors influencing response.
Figures
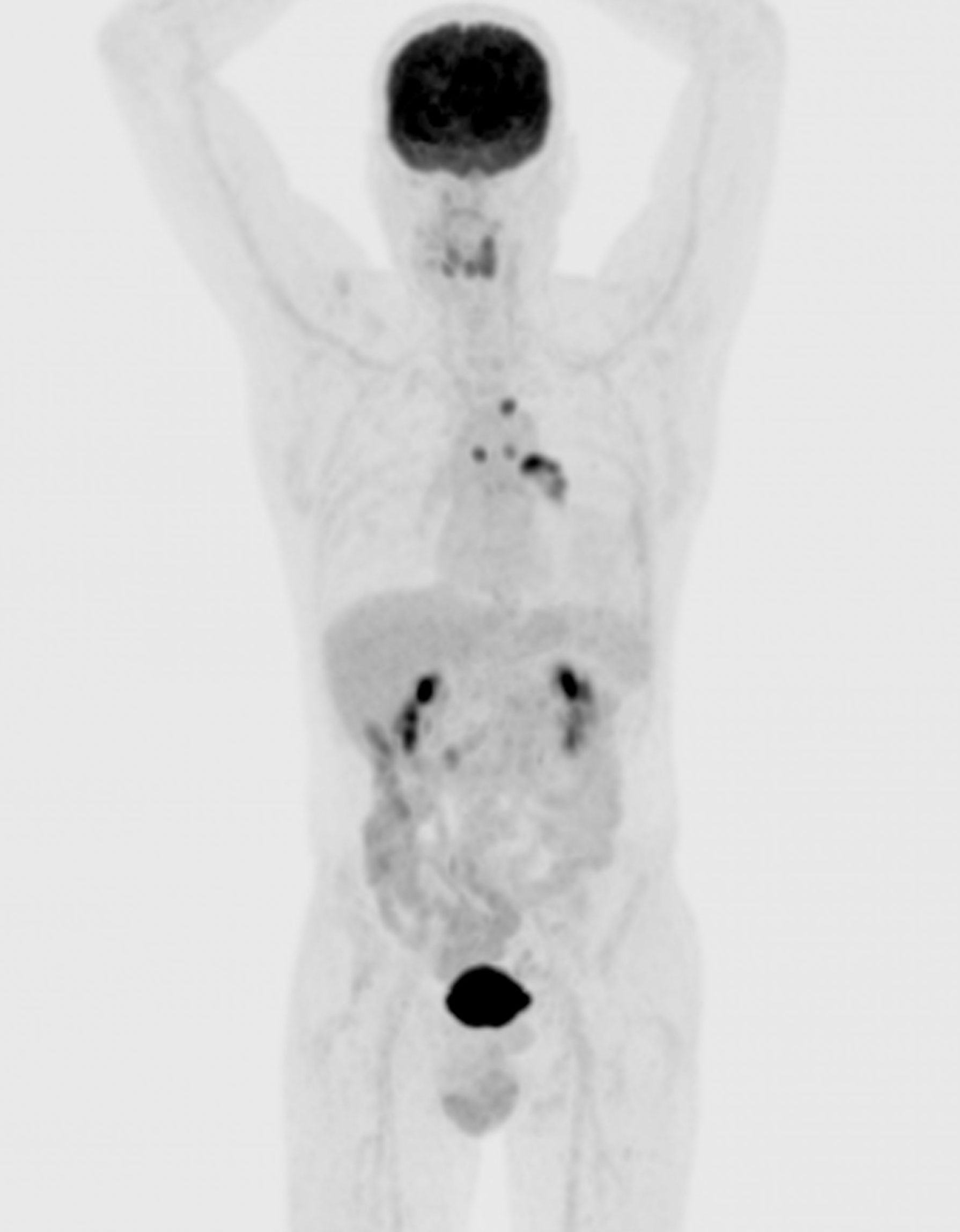
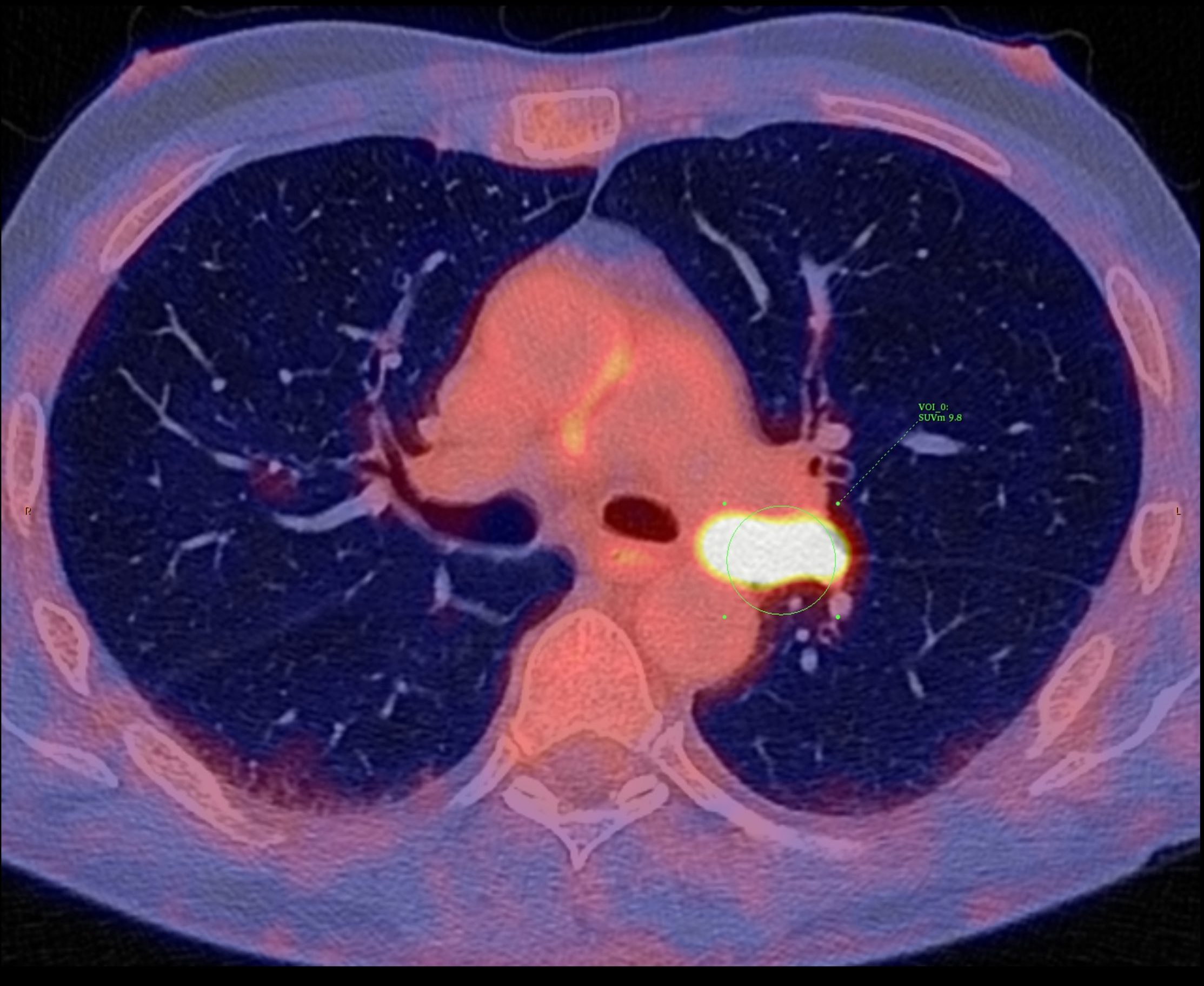
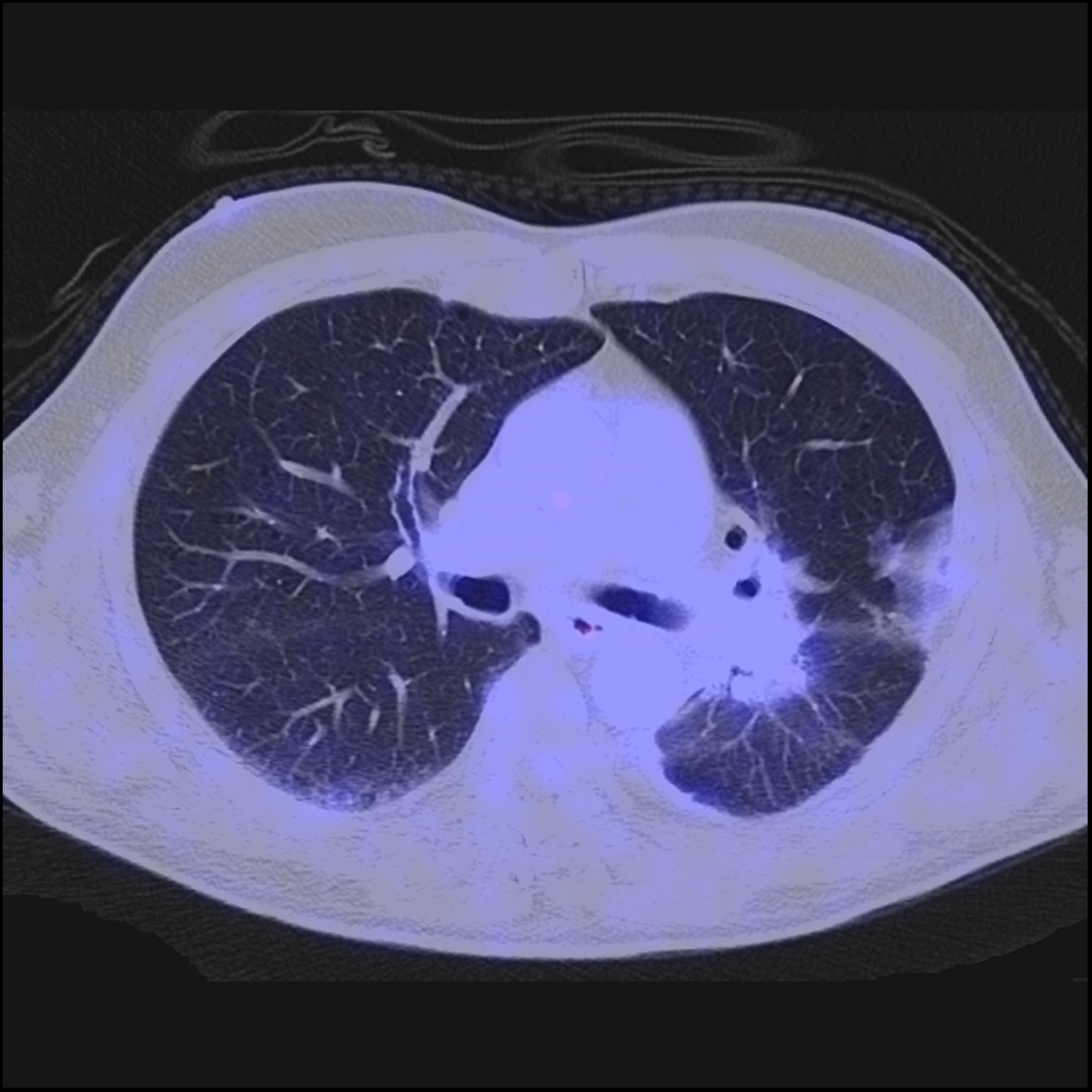
Figure 1A: 70M with NSCLC adenocarcinoma, left hilar primary tumour. Pre-treatment FDG PET/CECT shows intensely avid tumour, nodal and contralateral lung metastases. Tumour necrosis not a significant component in this case. Initial 3-month initial restaging PET/ CECT showed SUVmax reduction from 9.8 to 4.4 (>50%).
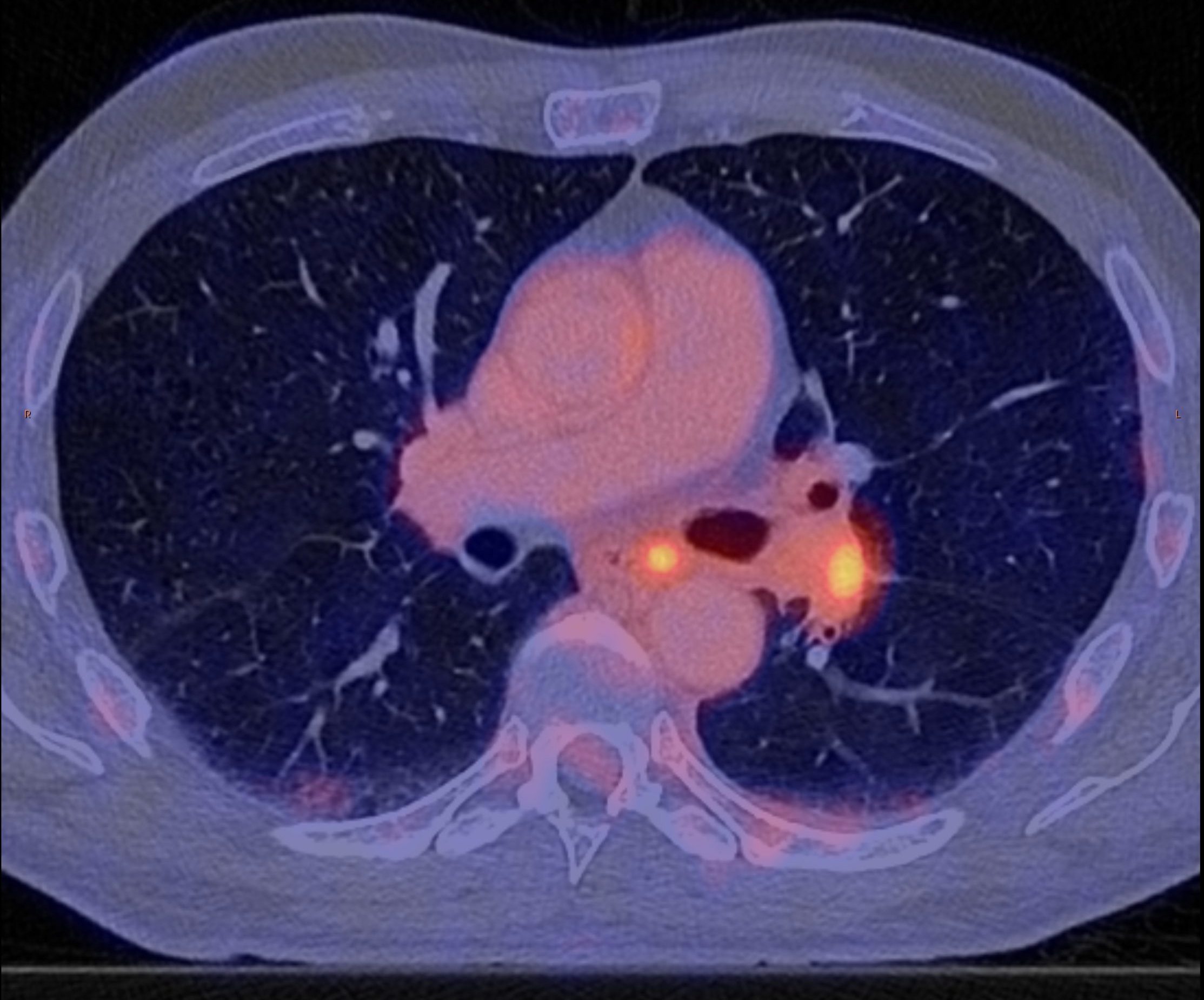
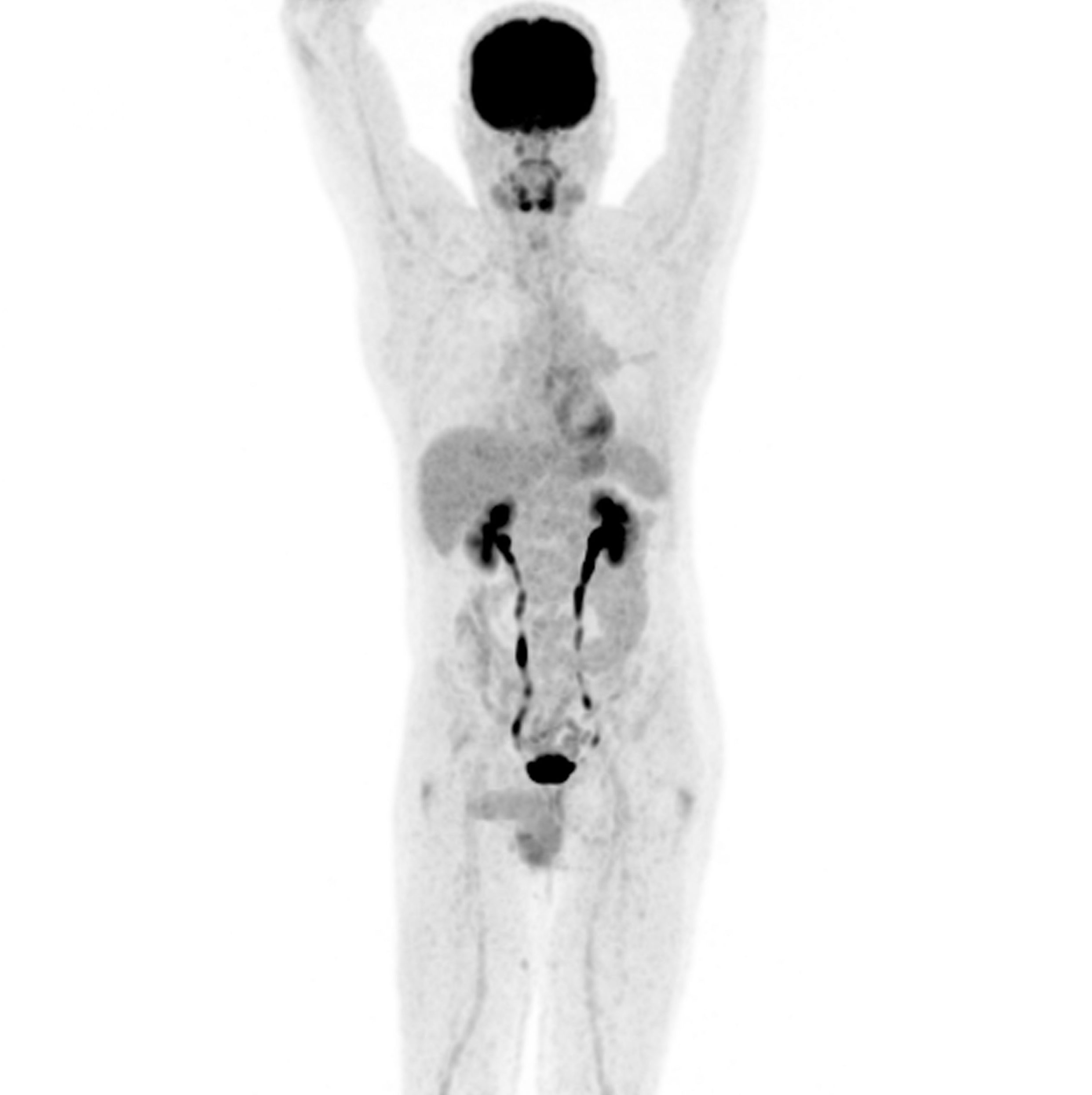
Figure 1B: At 12 months of follow-up, this patient shows complete sustained metabolic response to therapy. The magnitude of SUVmax response for the primary tumour and dominant node at the initial 3-month initial restaging PET/CECT study correlated to longterm immunotherapy response in this cohort.
References
Ferrari, C. et al. Immune Checkpoint Inhibitors in Advanced NSCLC: FDG PET/CT as a Troubleshooter in Treatment Response. Diagnostics 2021, 11, 1681. Curabitur ullamcorper ultricies nisi. Nam eget dui.
Lopci, E. et al. PET/CT Variants and Pitfalls in Lung Cancer & Mesothelioma. Sem Nuc Med 2021 51: 458-473.
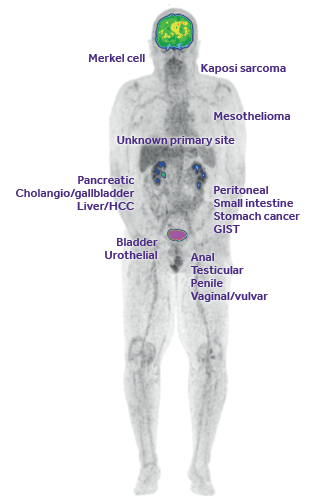
As of 1 November 2022, Medicare rebates are available for patients suffering from rare and uncommon cancers. These are cancers with an incidence of 12 or fewer per 100,000 people, and include those shown in the image below.
PET-CT scans are regularly used overseas to stage cancers to facilitate more accurate diagnoses and more informed treatment plans for oncologists and patients.
Qscan is a leader in PET-CT, consistently delivering a comprehensive diagnostic and therapeutic service for over a decade. Qscan has also been involved in pioneering rural and regional access to PET-CT services, and has built a reputation of being on par with Australia’s leading tertiary academic institutions in terms of referrer demand and case complexity.
More specific information regarding these Medicare changes is available from Medicare. For more information regarding the efficacy of PET-CT scans in the management of these cancers, click here for a range of case studies.
Qscan Group is committed to supporting the health and well-being of our teams, and this year, we held the first-ever national Q-FIT event on Sunday 11 September.
Q-FIT aimed to bring teams together from across the country by encouraging everyone to exercise at the same time on the same day – either by walking, running, or cycling. Q-FIT was designed to get our teams moving, fit and build workplace relationships.
We had mostly beautiful weather across the 17 national Q-FIT events, and the rain even held off in Hobart (although the “apparent temperature” was only 4.8 degrees so good on the Tassie teams for getting out there!)
A big shout out to the audit team who rocked up to the Brisbane event in purple tutus and to the Young team who had to change their course as their original waterfall course was too flooded.
Check out all of our events around the country!
National Q-FIT Events
Adelaide
Ballina
Brisbane cycle
Brisbane run or walk
Canberra
Dalby
Grafton
Gunnedah
Gold Coast
Hobart
Inverell
Katoomba
Mackay
Perth
Sydney
Tamworth
Young
Thank you to everyone who participated and got out and about over the weekend. We can’t for 2023’s Q-FIT event!
Radiofrequency ablation (RFA) is an interventional procedure performed by a high trained Radiologist under imaging guidance. It is a great tool for managing chronic pain and is effective at treating neck, back, knee, shoulder, and hip pain. It is suitable in patients who have previously had short lived or little response to steroid injections. Most of the patients treated with this procedure are at an end stage when it comes to their pain and have found this procedure useful in delaying or avoid surgery.
This procedure can provide long-term pain relief ranging from 6-18 months. A radiofrequency ablation aims to improve neck, back and joint pain so patients can reduce the amount of pain medication they are taking and to help improve their daily quality of life.
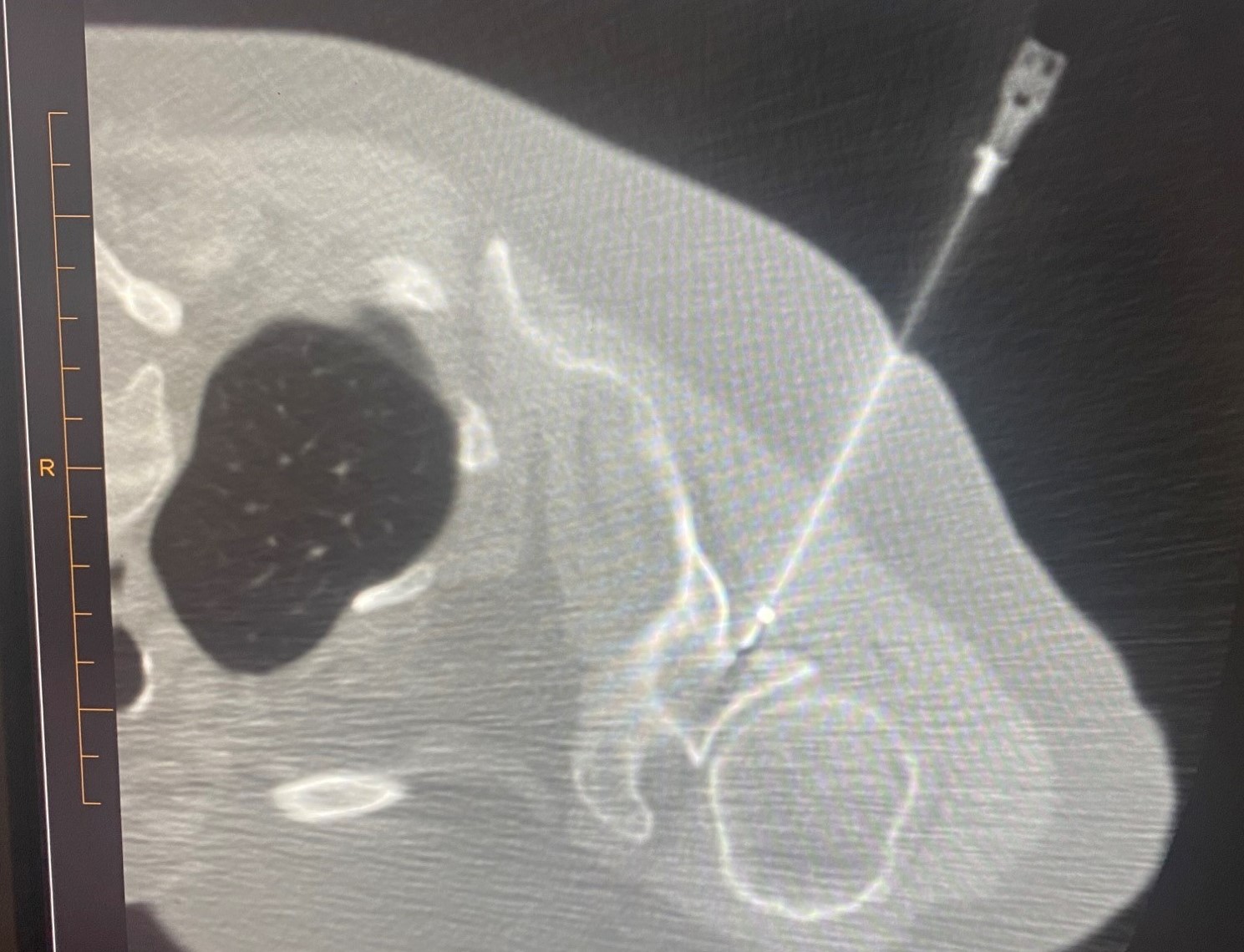
This interventional procedure targets the nerves that are causing pain by using radiowaves to generate a current through carefully placed needles. The needles are connected by insulated wires to grounding pads, which are attached to the patient’s back or thigh, and a generator. The current from the generator heats the tips of these needles, which can then stop nerves from sending pain signals to the brain.
There are two different types of radiofrequency ablation – continuous and pulsed. Continuous radiofrequency uses high voltage current to generate heat up to 80°C for 90-110 seconds to break down nerves, while pulsed radiofrequency ablations are conducted at a lower temperature of 42°C and help modulate the nerve function whilst preserving motor function.
Nerve tissue will regenerate after this procedure, but this can often take 18 months. If this happens, the pain associated with the nerve may also return. This is usually managed by repeating the procedure, and the procedure can be conducted as often as needed.
RFA procedure under CT guidance
At Qscan, we provide continuous and pulsed radiofrequency ablations as an in-patient service. They are performed with under local anaesthetic by a radiologist under imaging guidance. They are minimally invasive, and patients are usually able to return home on the same day as the procedure.
If you think you may benefit from a radiofrequency ablation, speak to your doctor about your suitability for this procedure. Radiofrequency ablations are offered at select Qscan clinics.
As of 1 July 2022, Medicare rebates are available for patients suffering from prostate cancer. Medicare will now cover the cost of whole body PSMA PET-CT scans for initial staging of prostate cancer, as well as restaging for prostate cancer recurrence.
More specific information regarding these Medicare changes is available from Medicare.
Qscan is a leader in PET-CT, consistently delivering a comprehensive diagnostic and therapeutic service for over a decade. Qscan has also been involved in pioneering rural and regional access to PET-CT services, and has built a reputation of being on par with Australia’s leading tertiary academic institutions in terms of referrer demand and case complexity.
Qscan Group was the first in Australia to use Fluorine-18 (F-18) in PSMA PET-CT scans. This tracer developed by Professor Martin Pomper, director of nuclear medicine and imaging at the Johns Hopkins University School of Medicine. To learn more, click here.
One of our excellent doctors, Hal Rice, has been named Gold Coast Australian of the Year from a very prestigious panel of finalists.
Hal is an incredible doctor, with achievements as a neurointerventionalist in the public and private systems. He is one of Qscan Queensland’s founding partners and established the renowned Neurointerventional Department at the Gold Coast Hospital.
He has been previously recognised by the City of Gold Coast for his work in promoting the city as an internationally acclaimed centre for innovations in stroke diagnosis, treatment, and research. His continued efforts to bring international medical conferences to the Gold Coast support the community at large and allow the city to uphold its credentials as a centre of medical excellence.
This award is a wonderful recognition of Hal’s contribution to neuroradiology, excellence in patient care, and his pivotal role in establishing the Gold Coast as a premier site for the endovascular treatment of life-threatening brain aneurysms and acute ischaemic stroke.
Congratulations Hal, a wonderful recognition of your contribution to Neuroradiology, excellence in patient care and establishing your city as a premier site for endovascular treatment of life-threatening brain aneurysms and acute ischaemic stroke.
Dr Hal Rice and Gold Coast Mayor Tom Tate at the Gold Coast Australian of the Year Awards night.
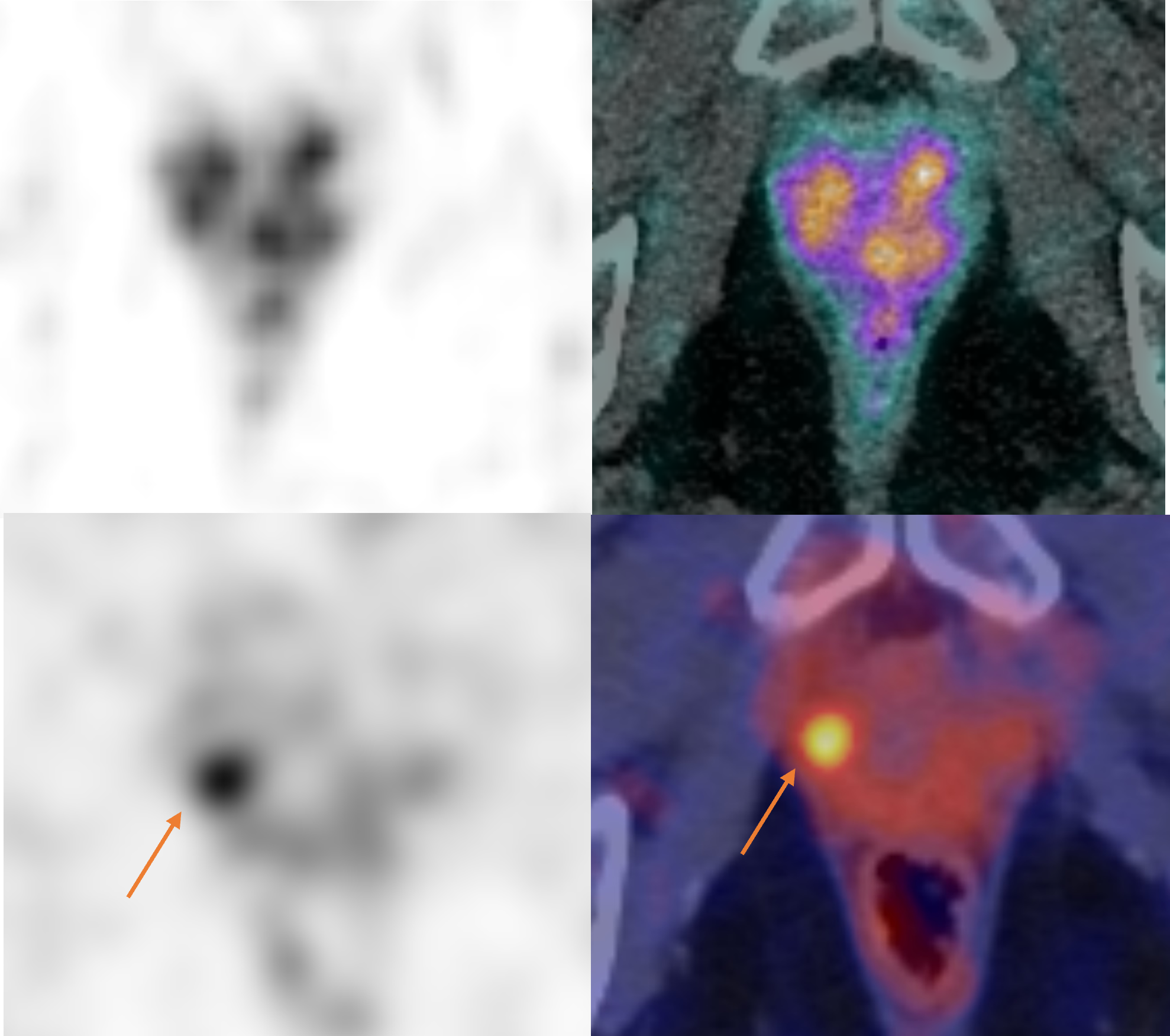
PSMA PET-CT scans are important in the detection and staging of prostate cancer. In Australia, the most commonly used tracer for PSMA PET-CT scans is Gallium-68 (Ga-68).
However, Qscan Group uses Fluorine-18 (F-18), a tracer developed by Professor Martin Pomper, director of nuclear medicine and imaging at the Johns Hopkins University School of Medicine.
Benefits of F-18
Improved image quality compared to scans using Ga-68
Intrinsic physical properties, which lends an improved spatial resolution of 5mm
Longer half-life, meaning increased reliability as a tracer
Lower urinary excretion
Improves detection of recurrences and additional lesions
Improved specificity in staging
Higher tumour uptake
High sensitivity, even in small tumours
Improved confidence for EPE and SVI
An 83-year-old male with a large basal PZ tumour. SVI is not clear in the Ga-68 PSMA images (note resolution and background noise), but with F-18, SVI is clearly resolved.
Reduced false positives for M staging
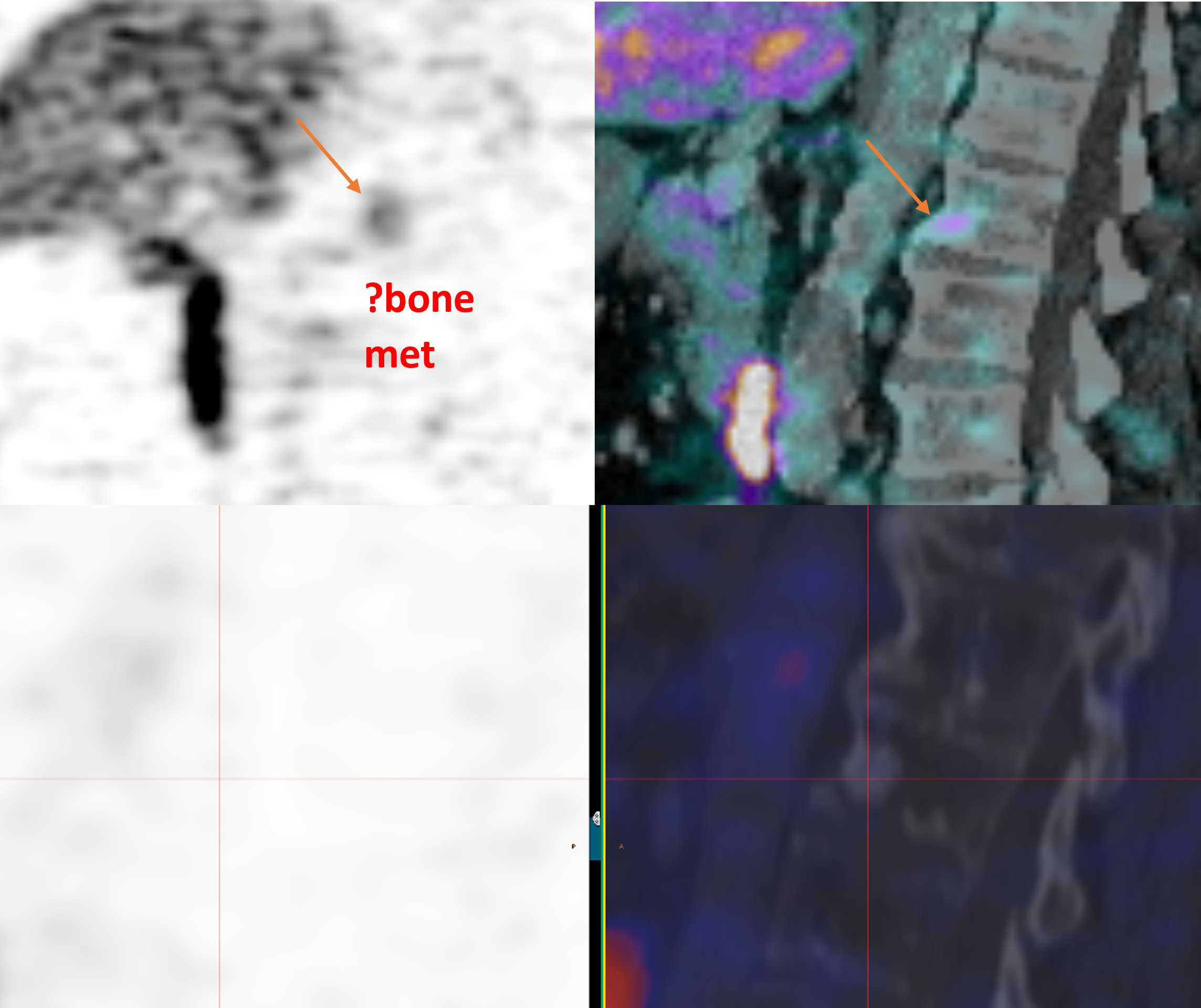
Scans of a 67-year-old male showing uptake in an L2 vertebral sclerotic lesion. Ga-68 PSMA (left) only showed background noise, while F-18 PSMA (right) allowed the patient to be cleared of metastatic disease.
Qscan Group has been using F-18 as our PSMA tracer of choice since 2017.
We are the most experienced in Australia when it comes to using F-18 for PSMA imaging, and will bring this leading expertise to all your prostate patients.
·Brauchli D, Singh D, Chabert C, Somasundaram A, Collie L. Tumour-capsule interface measured on 18F-DCFPyL PSMA positron emission tomography/CT imaging comparable to multi-parametric MRI in predicting extra-prostatic extension of prostate cancer at initial staging. J Med Imaging Radiat Oncol. 2020 Dec;64(6):829-838.
·Parathithasan N, Perry E, Taubman K, Hergarty J, Talway A, Wong L, Sutherland T. Combination of MRI prostate and 18F-DCFPyl PSMA PET/CT detects all clinically significant prostate cancers in treatment-naive patients: An international multicentre retrospective study. J Med Imaging Radiat Oncol 2022 Feb
FET PET-CT is a scan that can detect brain tumours – both primary and metastatic. FET PET-CT is indicated in the use of imaging of brain metastases as follows
Detection of viable tumour tissue; Radiolabelled amino acid imaging is superior to FDG PET, CT and MRI for differentiation of viable tumour tissue from treatment induced non-malignant changes such as post-operative change, oedema or radiation necrosis. FET PET is also superior to FDG PET for low grade recurrence.
Tumour Delineation; superior for estimation of true tumour extension in both low and high-grade gliomas.
Selection of biopsy site; FET is recommended to guide stereotactic biopsy for classification and grading of glioma.
Non-Invasive tumour grading; FET PET may aid in differentiating high grade gliomas from histologically benign brain tumours or non-neoplastic lesions. Oligodendroglioma and oligo-astrocytoma could have greater uptake than high grade gliomas.
Therapy Planning; FET PET used in conjunction with anatomical imaging may better define tumour volumes for resection of radiation therapy.
Tumour response; FET PET may predict the response to chemo and radiation therapy as it allows for earlier detection of residual tumour post-surgery.
Radiolabelled amino acids offer improvement over anatomical imaging (CT/MRI) as well as FDG PET-CT due to the low uptake of amino acids in normal brain tissue and therefore may be more tumour specific as uptake is less impacted by inflammation (1,2)
1.EANM Procedure Guidelines for Brain Tumour Imaging using Radiolabelled Amino Acid Analogues, Vander Borght et al 2006
2.Impact of F18-Fluoro-ethyl-tyrosine PET Imaging on target definition for radiation therapy of high-grade glioma, Rosenschold et al, Neuro-Oncology, Vol 17, Issue 5, May 2015.